FAQ
Quickly boost your growth with our Q&A section
Can't find the answer to your question? Message us on WhatsApp!
Below are answers to frequently asked questions
Most patients use crutches or a walker for two to five months after surgery (for 8-centimeter femurs and 5-centimeter tibias). A wheelchair is required for travel over long distances. In our physical therapy department, we teach patients how to partially bear weight on the limb.
Soft tissue serves as the limit for lengthening. The risk of complications associated with lengthening increases as the length increases.
Dr. Paley has conducted extensive research on this topic. Lengthening by up to 5 cm carries a low risk. Lengthening by 5 to 8 cm carries a moderate risk, and lengthening by more than 8 cm carries a high risk. For example, to achieve a 10 cm lengthening, it is much safer to lengthen the femur and tibia by 5 cm each than to lengthen each of these bones by 10 cm.
The price does not include implant removal (link to the price list for the implant removal section). The price for lengthening includes all additional auxiliary procedures, such as iliotibial band (ITB) release and biceps femoris tendon lengthening to lengthen the femur, as well as locking screws if needed for tibial lengthening, as well as peroneal nerve decompression in cases of tibial lengthening followed by femoral lengthening. These additional procedures are intended to PREVENT complications and do not incur an additional fee. Fortunately, complications requiring surgical intervention are rare. In approximately 1% of patients, complications arise that require unplanned surgery.
Please schedule an appointment at the Paley Lengthening Center by calling +48 22 150 15 13 or emailing recepcja@paleyeurope.com.
Unlike other plastic surgery procedures, limb lengthening can lead to chronic pain. Therefore, the most important factor to consider is not cost, but safety.
There are many centers around the world that offer limb lengthening at lower prices than the Lengthening Center. Safety is the most important factor when choosing where to undergo the procedure. Safety stems from experience and good organization. Our multidisciplinary, well-organized team consists of surgeons, anesthesiologists, physicians, nurses, physician assistants, physical therapists, occupational therapists, orthopedic technicians, and patient coordinators. All of them are dedicated to the limb-lengthening process, ensuring it is safe, reliable, and as efficient as possible. Our team is available 24 hours a day, 7 days a week, 365 days a year, to provide care to all our patients from around the world
- Hospital stay of up to 2–4 days.
- All hospital charges related to the operating room and recovery room.
- Cost of implants: 2/4 PRECICE screws.
- Anesthesiologist fees.
- Surgeon's fees.
- Surgical assistant fees.
- Hospital physician fees.
- Radiologist's fee (includes the fee for interpreting all X-ray images).
- All diagnostic tests performed at the hospital upon admission.
- All X-rays.
- All in-office visits.
- Transportation to and from the Institute for medical consultations and physical therapy.
- A wheelchair, walker, crutches, and a bedside commode, if needed after surgery, are provided upon discharge from the hospital.
- Physical therapy.
- >Removal of implants.
- >Medications and pharmaceutical products (e.g., pain relievers, anticoagulants, dietary supplements such as calcium and vitamin D, anti-inflammatory drugs).
- >Meals after discharge from the hospital.
- >Home care.
- >Additional physical therapy.
Full payment is required one month before the surgery; otherwise, the procedure will be canceled. Payment can be made by bank transfer.
We use a minimally invasive method to insert the bone lengthening device. We make an incision 1 to 1.5 cm long in the hip area and about five 6-mm (0.25-inch) incisions on the lateral surface of the thigh. These scars are so small that they are barely visible. Most of them look no bigger than a mosquito bite. For the tibia, we make one 12-mm (0.5-inch) incision and eight 6-mm (0.25-inch) incisions. The incision through the fibula is about 2–3 cm long, and the fibular nerve decompression incision is about 4 cm long.
Postoperative pain occurs immediately after the procedure. The procedure is performed under general anesthesia. After the procedure, the patient receives intravenous pain medication in the hospital to relieve pain. Some patients may use PCA or epidural anesthesia for pain relief. We often inject a long-acting, slow-release local anesthetic (Exparel) into the incisions, which lasts for 96 hours. These methods provide excellent control of postoperative pain. Patients transition to oral pain medications in preparation for discharge from the hospital. Upon discharge, all patients receive a prescription. For the first two weeks after surgery, most patients continue to experience postoperative pain. Once the pain subsides, comfort improves significantly. The most painful moments occur during stretching exercises, physical therapy, and before bedtime. Most patients do not complain of severe pain during the day. The lengthening process itself is usually painless. Most patients experience little or no pain most of the time.
-> Information: Review the provided materials (print and online).
-> Consultation: Schedule an appointment to address any concerns in person.
-> Activity: Incorporate regular stretching exercises.
-> Medications and Supplements: Stop taking anti-inflammatory medications, aspirin, and fish oil one month before surgery.
-> Stimulants (key): Completely stop smoking and vaping (including secondhand exposure) at least 3 months before the procedure.
-> Time: Set aside at least 3 months for your stay in Warsaw.
-> Work: Plan your leave so as to avoid the pressure of returning to work.
-> Budget: Set aside funds for the surgery itself and an additional reserve in case of rare but costly complications.
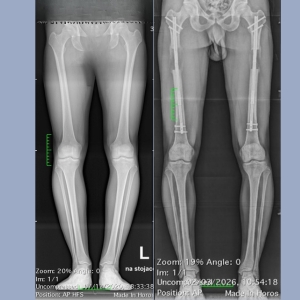
The consultation begins with a specialized standing X-ray, known as an EOS scan. This is a low-dose, full-body scan from head to toe, performed in two planes (front and side simultaneously). You will meet with one of our physician assistants, as well as Katarzyna Zawadzka. You will then meet with Dr. Deszczyński and Dr. Albrewczyński. The specialists will assess your health and analyze the X-rays. The examination will include joint range of motion, muscle tone, as well as measurement of height and body and bone proportions based on the EOS scan. The normal ratio of tibia to femur length is 0.80 ± 0.02. If this ratio is greater than 0.82, your tibia is relatively long compared to your femur, and femur lengthening may be preferred; however, if the ratio is less than 0.78, then tibia lengthening may be preferred. This should be taken into account because the femur can be safely lengthened by up to 8 cm, while the tibia is typically lengthened by up to 5 cm. A doctor will then meet with you to help tailor the lengthening option to your specific goals regarding height, body proportions, financial capabilities, and time availability.
Yes, during your appointment you will receive a surgical plan that you will need to follow. Before the surgery, you will meet with the surgical team to discuss the consent form and all documentation. You will also schedule an appointment with the anesthesiologist. Before the surgery, you can discuss anesthesia and postoperative pain management. You will also receive instructions regarding the procedure.
The hospital stay usually lasts 2–3 nights. The surgery takes place at Medicover Hospital, located about 500 meters from the Paley European Institute.
After the surgery, you will be taken to the recovery room for an hour or two before being transferred to your room. You will receive an intravenous iron infusion to help replenish blood loss and prevent the need for a transfusion. If you have family or friends, our patient liaison will keep them informed about the progress of your surgery. During your hospital stay, you will begin taking a blood-thinning medication to prevent blood clots. The nurses will ensure that you are comfortable and that your position is appropriate to prevent pressure sores. Blood tests will be performed to monitor your blood parameters. It is worth noting that even with low blood counts, the need for a transfusion is rare and affects only 2% of patients. Every day, our specialist nurses will come to check on you. You will also see the rest of the surgical team, as well as Dr. Deszczyński and Dr. Albrewczyński. If epidural anesthesia or PCA is used, it is usually discontinued after two days. A physical therapist will visit every day to teach you how to move around and become more independent. You will learn skills such as transferring between your wheelchair and the toilet. Once you are mobile enough, you will be discharged from the hospital and given instructions on how to proceed.
We rarely give patients blood transfusions after surgery. We administer iron intravenously to all patients to raise their blood iron levels more quickly. Very few patients lose enough blood to require a transfusion before surgery. If necessary, we use blood from a blood bank. Blood loss occurs not only during surgery but also afterward, for several days. If a transfusion is necessary, it almost always takes place one or two days after surgery. The associated risk is minimal. Less than 2% of our patients require a transfusion.
Yes, you will be provided with a wheelchair and a walker, which you can take with you. Our medical care coordinator will arrange everything for you. Our hospital physical therapists will teach you how to transfer from your bed to a chair and to the restroom. At first, you will use the walker, and later you will be able to use crutches.
Blood thinner to prevent blood clots: Xarelto 10 mg daily (about $625 per month). Pain medication (as needed): Percocet 5/325, 90 tablets for 7 days (approximately $60); we will refill the prescription as needed during extended treatment. Due to the opioid crisis, in accordance with new laws, you must schedule an appointment with our doctor to refill this prescription. Muscle relaxants, vitamin D, and anti-inflammatory medications are also used as part of the treatment.
It is up to the patient to find an apartment, hotel, or house to rent, preferably as close as possible to the hospital and the Institute.
You must remain in the clinic until the end of the distraction (lengthening) phase. The duration of the distraction phase for femoral lengthening is one day for every millimeter of planned lengthening. For example, 80 mm = 80 days. Lengthening begins only 7 days after surgery. Therefore, 80 days for 80 mm plus 7 days = 87 days (12 weeks) for 80 mm. Tibia lengthening is 0.75 mm per day compared to 1 mm per day for femur lengthening. For tibia lengthening, the distraction phase for 50 mm lasts 10 weeks plus 1 week before the start of lengthening; a total of 11 weeks.
Yes, you’ll need to either come with someone who can take care of you or hire a caregiver for the first two to three weeks. We can provide you with the contact information for a home health aide. You’ll need more hours of assistance during the first week after you’re discharged from the hospital, and less as time goes on. You’ll need to factor this into your budget if you’re coming on your own.
Patients undergoing implantable limb lengthening surgery may only drive vehicles with automatic transmissions, provided they do not use drugs during the day, and depending on how the recovery process is progressing and the patient’s sensation in the limbs. However, they must be able to get in and out of the car on their own. They must be able to stand up on their own with the aid of crutches or a walker, and then transfer to a wheelchair on their own to achieve full independence. They must learn how to do this and be able to perform these tasks while adhering to the above WB restrictions.
Every day, 5 days a week, throughout the lengthening phase. During the consolidation phase, the patient must continue physical therapy, but less frequently (2–3 days a week). This is usually done closer to home, as most patients leave the Paley European Institute and return home. If you plan to stay in the area longer, we can arrange physical therapy at our center. The additional cost can be paid weekly. Daily exercises at home are required of the patient during both the distraction and consolidation phases.
The patient or their caregiver performs the lengthening at home. Lengthening is performed in 0.25 mm increments, 4 times a day for the femur and 3 times a day for the tibia. In the case of simultaneous lengthening of the femur and tibia, the femur is lengthened 3 times a day and the tibia 2 times a day. Lengthening is performed using a special ERC (External Remote Control) device. Our orthopedic technician teaches each patient how to use the ERC device until they feel comfortable with it. Each patient receives an ERC device that they can take home with them.
Every two weeks after the lengthening process begins, you will have a follow-up appointment at the Paley Lengthening Center with the medical team.
Every two weeks after the lengthening process begins, X-rays are taken of each bone being lengthened. These X-rays are also taken during the follow-up visit.
You can go home right after the implant is removed.
Send X-rays to Dr. Deszczyński and Dr. Albrewczyński every month. There are several ways to send X-rays. Your medical care coordinator will inform you of the available options.
Health insurance does not cover any cosmetic procedures. Cost is the main obstacle for most people interested in bone lengthening for cosmetic reasons. Not only does insurance not cover the cost of the procedure itself, but in the event of complications requiring additional surgery, insurance will not cover the cost of treating those complications either.
After reviewing the X-rays, your doctors will discuss the results with you and let you know whether you can return to full hip stability. This usually occurs one to two months after the end of distraction. Most patients can return to full hip stability one to two months after a 5-cm femur lengthening and two to three months after a 5-cm tibia lengthening. Most patients can return to full hip stability two to three months after an 8-cm femur lengthening.
To return to sports, you need to regain your range of motion and then build up your muscle strength. If you work hard at it, you can be back in shape as early as six months after surgery. Your doctor will determine this on a case-by-case basis for each patient.
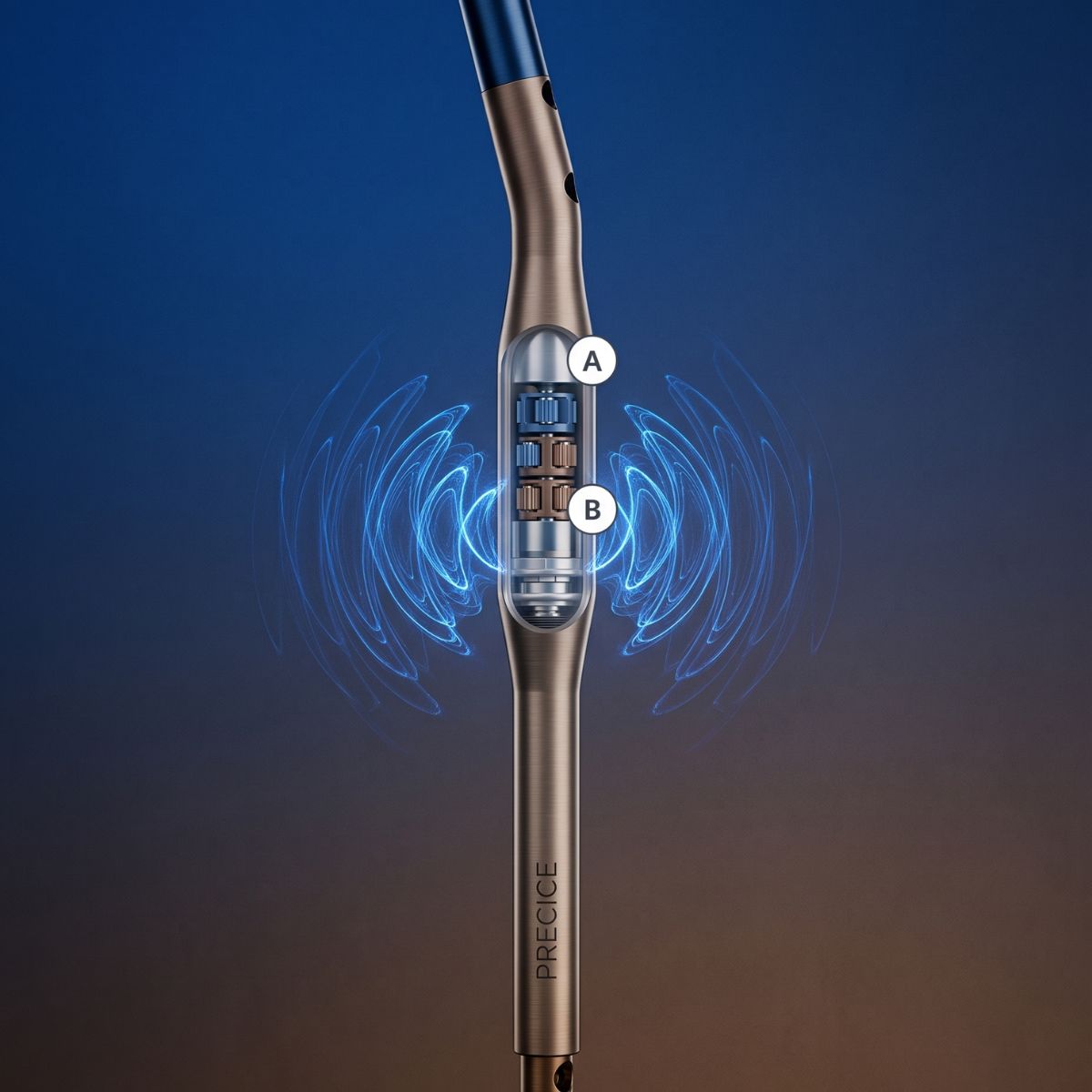
Yes, all implants should eventually be removed. This usually takes place one to two years after the procedure. Although this is not an urgent procedure, it is recommended because the moving metal parts of the nail may release metal ions over time. Additionally, the device contains a neodymium (rare-earth) magnet enclosed in a sealed chamber. To avoid the risk of this chamber becoming compromised by bodily fluids after many years, it is better to remove the implant as a preventive measure.
The cost of implant removal is separate and not included in the treatment price. Removal costs 25,000 PLN/9,900 EUR for bilateral femoral bone removal, PLN 25,000/€9,900 for bilateral tibial bone removal (including tibiofibular screws and locking screws), and PLN 45,000/€17,820 for simultaneous bilateral removal of the femur and tibia.
If you decide to undergo a second lengthening procedure, a 12-month interval between procedures is recommended. It is possible to lengthen both the femur and the tibia at the same time; this option should be discussed with your doctor.
We take a very conservative approach to many aspects of the limb-lengthening process. We strive to anticipate potential problems and prevent complications. Many complications result in the need for additional surgeries, and thus additional costs. The link below provides a list of some potential complications:
We provide preliminary information electronically, but an in-person evaluation during the consultation is always necessary. This allows us to optimally prepare the patient for the procedure and carry out all necessary steps.
The first-generation PRECICE method was developed by Ellipse Technologies in collaboration with a team of orthopedic surgeons, including Dr. Paley. This method was designed to treat limb length discrepancies. Dr. Paley was the first physician in the United States to implant a P1 nail. This took place on December 1, 2011. The second-generation PRECICE nail (P2) was developed through a collaboration between Dr. Dror Paley and Ellipse Technologies, primarily with the needs of patients seeking to increase their height in mind. It is thus the first intramedullary nail designed specifically for the requirements of a cosmetic procedure. The P2 model was first used by Dr. Paley in November 2013. The P2 allows for an 8 cm lengthening using an implant available in three sizes: 8.5 mm, 10.7 mm, and 12.5 mm in diameter. The 8.5 mm diameter nail is intended for smaller bones, such as those typically found in children, patients with dwarfism, and adults with a slender build. The P2 nail also features a structure that is nearly four times stronger, allowing for greater load-bearing capacity. In addition, the strength of the telescopic joint has been increased nearly threefold, which reduces the risk of nail mechanism failure in cases of excessive bone tissue formation, preventing complications of premature union (bone tissue healing) that can halt the lengthening process. In short, Precice2 allows for a greater range of lengthening thanks to a stronger design with a more durable piston. The P2 is available in several sizes and accommodates different patient body types. The latest modification to this model involved reinforcing the connection between the two telescopic ends of the nail. There is a special welded joint called a crown, which in rare cases failed, increasing the risk of nail fracture. It was Dr. Paley who identified this flaw and worked with the manufacturer to eliminate it, further strengthening the product’s design. The P2.1 model was launched in December 2014, and the P2.2 in May 2015, replacing all previous P2 models. The P2.2 nail is even stronger and more resistant to any defects or breakage. Ellipse was acquired by Nuvasive. The product is currently sold by Nuvasive Specialized Orthopedics.
The price of the femur and tibia lengthening procedure includes all additional accompanying procedures, such as iliotibial band release and biceps femoris tendon lengthening during femur lengthening, or any locking screws used during tibia lengthening. These procedures are intended to PREVENT complications. The necessity of performing them is determined during the initial consultation. Without examining the patient, it is impossible to determine whether and which procedures will be necessary. The greater the extent of the lengthening, the higher the likelihood that soft tissue reconstruction will be necessary. To illustrate, every patient undergoing 8 cm of bone lengthening requires ilio-tibial band reconstruction, whereas for 5 cm of lengthening, this is necessary in only 50% of cases. In the case of tibial lengthening, if the Silverskold test (during the physical examination) reveals excessive tension in the Achilles tendon, the procedure may result in a contracture of the triceps surae muscle. Although a repair is performed, it can lead to permanent weakening of the push-off force. We avoid such situations and limit the extent of tibial lengthening.
If excessive tension is already present before surgery and prophylactic plasty is not performed, muscle/joint contractures will require more costly procedures at a later date. Concurrent with tibial lengthening, prophylactic anterior compartment plasty may be performed to prevent compartment syndrome.
Fortunately, complications requiring surgical intervention are rare. Unplanned complications occur in approximately 4% of patients.
We provide preliminary information via email, but an in-person evaluation during a consultation is always necessary.
This allows us to optimally prepare the patient for the procedure and carry out all necessary steps.
The consultation begins with a specialized X-ray examination using the equipment available at the Paley European Institute.
First, the patient will meet with a medical assistant. A detailed medical history is taken. Measurements of height, weight, and arm span are also taken.
Next, a medical team reviews the X-rays and examines the patient, including a physical examination to assess range of motion and muscle tone. They explain the procedure and recommend the best lengthening strategy for the patient, taking into account their individual expectations and body proportions. Based on the radiological examination, the medical team calculates the bone length ratios. The normal ratio of the tibia to the femur is 0.80 ± 0.02. If this ratio is greater than 0.82, it means that the tibia is relatively long compared to the femur, and femoral lengthening will be recommended. Conversely, if the ratio is below 0.78, tibial lengthening will likely be recommended. An additional criterion here is the expected gain in length, as up to 8 cm can be safely achieved in the femurs, whereas only 5 cm is possible in the lower legs. The medical team will discuss these and other aspects of the procedure in detail and then answer all your questions.
After the medical consultation, a medical assistant stays with the patient to answer any additional questions. The patient also tours the physical therapy department with them. Whenever possible, the patient also has the opportunity to speak with other patients undergoing limb-lengthening procedures. We cannot guarantee this, however, as patients are scheduled for physical therapy independently of the consultation schedule.
They must also consent to such a meeting. We respect the privacy of all patients and guarantee them discretion.
X-rays should be sent to the Paley European Institute every month, where Dr. Deszczyński and Dr. Albrewczyński will assess the progress of bone remodeling. It is best to send them by email to: badania@paleyeurope.com.
If you have trouble attaching an X-ray image to an email, you can send a disc containing the image(s) to the following address: Paley European Institute, 1 Aleja Rzeczypospolitej, 87-100 Warsaw
The process of lengthening the femurs by 8 cm takes three months, followed by another 2–3 months for the bone tissue to heal to a state that allows for full weight-bearing on the limb without crutches; this totals 5 months. The procedure for lengthening the femurs by 5 cm takes just under 2 months. In the case of the PRECICE nail, an additional month or two must be added to this. After this time, it will be possible to bear full weight on the limbs without crutches. In the case of the tibia, lengthening by 5 cm takes three months, while it takes another 2–3 months for the bone tissue to heal to a state that allows walking with full weight-bearing without crutches.
The extent of lengthening is limited by the capacity of the soft tissues. The risk of complications from the lengthening procedure increases with the length of the limb. Lengthening up to 5 cm is a low-risk procedure. In the 5–8 cm range, the risk is moderate, and above 8 cm, it is high. For example, to gain an additional 10 cm in height, it is much safer to lengthen the femur and tibia by 5 cm each than to lengthen either one by 10 cm.
The first-generation PRECICE method was developed by Ellipse Technologies in collaboration with a team of orthopedic surgeons, including Dr. Paley. This method was designed to treat limb length discrepancies.
Dr. Paley was the first physician in the United States to implant a P1 nail. This took place on December 1, 2011. The second generation of the PRECICE nail (P2) was developed through a collaboration between Dr. Dror Paley and Ellipse Technologies, primarily with the needs of patients seeking to increase their height in mind. It is therefore the first intramedullary nail designed specifically for the requirements of a cosmetic procedure. The P2 model was first used by Dr. Paley in November 2013. The P2 allows for an 8 cm lengthening using an implant available in three sizes: 8.5 mm, 10.7 mm, and 12.5 mm in diameter. The 8.5 mm diameter nail is intended for smaller bones, such as those typically found in children, patients with dwarfism, and adults with a slender build. The P2 nail also features a structure that is nearly four times stronger, allowing for greater load-bearing capacity. In addition, the strength of the telescopic joint has been increased nearly threefold, which reduces the risk of nail mechanism failure in cases of excessive bone tissue production, preventing complications of premature union (bone tissue healing) that can halt the lengthening process. In short, Precice2 allows for a greater range of lengthening thanks to a stronger design with a more durable piston. The P2 is available in several sizes and accommodates different patient body types. The latest modification to this model involved reinforcing the connection between the two telescopic ends of the nail. There is a special welded joint called a crown, which in rare cases failed, increasing the risk of nail fracture. It was Dr. Paley who identified this flaw and worked with the manufacturer to eliminate it, further strengthening the product’s design. The P2.1 model was launched in December 2014, and the P2.2 in May 2015, replacing all previous P2 models. The P2.2 nail is even stronger and more resistant to any defects or breakage. Ellipse was acquired by Nuvasive. The product is currently sold by Nuvasive Specialized Orthopedics.
The price of femoral and tibial bone lengthening procedures includes all additional associated procedures, such as iliotibial band release and biceps femoris tendon lengthening during femoral lengthening, or any locking screws used during tibial lengthening. These procedures are intended to PREVENT complications. The necessity of performing them is determined during the initial consultation. Dr. Paley performs four tests (the Ober test, popliteal angle assessment, the Ely test for femur lengthening, and the Silverskiold test for tibia lengthening) to assess muscle function and potential contractures: the iliotibial band/fascia lata, the ischio-tibial muscles, and the rectus femoris muscle during femoral lengthening, and in the case of tibial lengthening—the triceps surae muscle. Without examining the patient, it is impossible to determine whether and which procedures will be necessary. The greater the extent of lengthening, the higher the likelihood that soft tissue reconstruction will be necessary. To illustrate, every patient undergoing 8 cm of bone lengthening requires iliotibial band reconstruction, whereas in the case of 5 cm of lengthening, this is necessary in only 50% of cases. In the case of tibial lengthening, if the Silverskold test (during the physical examination) reveals excessive tension in the Achilles tendon, the procedure may result in a triceps surae contracture. Although a triceps surae release is performed, it can lead to permanent weakening of the push-off force. We avoid such situations and limit the extent of tibial lengthening.
If excessive tension is already present before surgery and prophylactic plasty is not performed, muscle/joint contractures will require more costly procedures at a later date. Concurrently with tibial lengthening, prophylactic anterior compartment plasty may be performed to prevent compartment syndrome.
Fortunately, complications requiring surgical intervention are rare. Approximately 4% of patients experience complications requiring unplanned interventions.
Health insurance does not cover any cosmetic procedures. Cost is the main obstacle for most people interested in bone lengthening for cosmetic reasons. Not only does insurance not cover the cost of the procedure itself, but in the event of complications requiring additional surgery, insurance will not cover the cost of treating those complications either.
The Paley Institute is the safest and most reliable center in the world for such procedures.
Prices vary depending on the country, the center, the specialist, and the method. A significant portion of the total cost of the procedure is attributed to the purchase of the device itself. An alternative is external fixators, which, although expensive, are reusable. Prices for used external fixators are very low. However, it should be emphasized that the experience of having a massive external fixator applied and then worn, with all the complications typical of such devices—such as infections, joint stiffness, or scarring— cannot be compared to a procedure using the latest, safest technology that minimizes scarring, adhesions, and stiffness, as well as the risk of infection and pain. Many patients choose to seek treatment abroad precisely because of the costs. In many facilities, the patient is at risk of permanent disability. It is very difficult for consumers to choose the right facility. Specialists performing limb-lengthening procedures vary in skill, as do the centers that employ them. Just because something is cheaper does not mean the patient will achieve the same desired result.
In our opinion, the rule that price reflects quality holds true in many cases. Precice is the most advanced and safest method of limb lengthening for cosmetic purposes, offering less pain and fewer complications than other procedures.
The Paley European Institute has the most extensive experience in the world with these procedures, made possible through ongoing collaboration with Dr. Dror Paley.
Dr. Dror Paley has the most extensive experience in limb lengthening surgeries, performed both to increase height and to correct limb length discrepancies. Since 1986, he has performed over 20,000 limb lengthening procedures. He boasts the highest success rate for all methods. This is of paramount importance for patient safety
In our opinion, the choice should be based on an analysis of four aspects. These are:
SECURITY,
EXPERIENCE,
CREDIBILITY,
REPEATABILITY.
Postoperative pain occurs immediately after surgery. Most patients receive epidural anesthesia. We often inject a long-acting local anesthetic into the wound, which remains in the body for up to 96 hours. These methods are highly effective in managing postoperative pain. While still in the hospital, patients begin taking oral pain medications. Upon discharge, all patients receive a prescription for pain medications and instructions on how to use them. During the first two weeks after surgery, most patients continue to experience some degree of postoperative pain. Once the pain subsides, the patient’s comfort improves significantly. The most intense pain occurs during stretching exercises as part of physical therapy and when falling asleep. For this reason, we sometimes prescribe sleep aids. Most patients do not report pain during the day. The Precice lengthening procedure itself is usually painless. Patients who have undergone the lengthening procedure report only mild pain.
It’s a good idea to start with some educational resources:
Check out our materials, schedule an appointment, and get answers to your questions during your visit:
Please send any additional questions via email.
Physical conditioning is also important. At the Paley European Institute, we were the first to introduce a coordinated, dedicated functional conditioning program for limb-lengthening procedures. Before treatment, each patient is evaluated by our team, which consists of doctors, a team of physical therapists, and physical conditioning coaches. Before the procedure begins, each patient undergoes an individualized preparation program to achieve the best possible therapeutic outcome, a quick return to full fitness, and to minimize the risk of complications.
Quit smoking and avoid exposure to secondhand smoke. Discontinue all anti-inflammatory medications.
Take care of practical preparations: Organize your life so that you can afford to take at least a 3-month break. Your stay in Warsaw will last at least 9 weeks. After returning home, you will still need to use a wheelchair for at least a month, so returning to work may not be possible.
Secure sufficient financial resources to cover not only the procedure itself but also the treatment of any potential complications. These do not occur often, but when they do, additional funds will be needed.
Prepare yourself mentally to focus on a single goal and devote all your attention and energy to the limb-lengthening process and rehabilitation.
Visit our Institute. Check out the place where you plan to stay and explore the surrounding area.
Arrange for assistance from a companion or be prepared to hire a housekeeper.
Notify your workplace of your absence (arrange for leave) so you don’t feel pressure to return.
Please schedule an appointment at the Paley European Institute by calling +48 22 150 15 13 or emailing recepcja@paleyeurope.com.
Following your consultation at the Paley European Institute, the PEI Medical Care Coordinators will be happy to answer any organizational questions you may have, outline the next steps, and schedule follow-up appointments, your surgery date, and your entire post-operative care plan.
Before the procedure, a preoperative consultation is held with the surgical team, during which consent forms and other necessary documents are completed. The patient also meets with the anesthesiologist. In addition, the methods of surgical anesthesia and post-operative pain management are discussed. The patient also receives recommendations regarding the procedure. This visit usually takes place a few days before the surgery.
Hospitalization usually lasts 3–4 nights. At the Medicover private hospital, patients over the age of 18 are accommodated in rooms within the Surgery Ward.
After the procedure, the patient is taken to the recovery room for an hour or two, and then to their room. If family or friends are present, our Medical Care Coordinators provide updates throughout the procedure and, once it is complete, arrange a meeting with Dr. Deszczyński and Dr. Albrewczyński. They then escort the family/friends to the recovery room, if the patient so desires. The patient has an IV line and a Foley catheter (bladder catheter) in place. The catheter remains in place until the epidural catheter is removed. If epidural anesthesia was not used, the Foley catheter is removed one or two days after the procedure. During the hospital stay, we begin administering anticoagulant medications. Nurses ensure the patient’s comfort and position them to prevent pressure ulcers. We draw blood for testing every morning. If the blood parameters are unsatisfactory, a transfusion may be ordered, though this is very rare. Epidural anesthesia is usually discontinued after two days. A physical therapist visits the patient daily to teach them how to move and regain independence. The patient learns new skills, such as transferring to a wheelchair or commode chair, returning to bed, etc. Once the patient has regained a satisfactory level of mobility and their pain has subsided, they are discharged from the hospital with follow-up instructions.
Some patients lose so much blood that they need a transfusion even before the procedure. It is possible to bank your own blood, but it is not required. If necessary, we use a blood bank. Blood loss occurs not only during surgery but also over the next few days. If a transfusion is needed, it most often occurs on the first or second day after the procedure. The associated risk is minimal. Less than 10% of our patients require a blood transfusion.
Anticoagulants: Clexane 40 mg daily,
Pain relievers (as needed) – prescriptions are provided upon request during the lengthening procedure,
Muscle relaxants (optional): Valium 5 mg.
Vitamin D and anti-inflammatory medications are also administered.
We offer several options. We recommend contacting the Patient Care Coordinator.
Yes – you will need assistance during the first 2–3 weeks. You should arrive with a companion who will take care of you. Alternatively, you can hire a caregiver for the first two or three weeks after surgery. We can help arrange this. During the first week after discharge, you will need more assistance than in the weeks that follow. If the patient arrives alone, they must provide for this need. Everyone needs assistance for at least two weeks after being discharged from the hospital. In the absence of a companion, the patient will require several hours of assistance per day.
During distraction, the bone ends are kept apart by an implanted intramedullary nail. It is secured in the bone tissue using screws at both ends. The diameter of the nail is 8.5, 10.7, or 12.5 mm. The diameter of the screws is 4–5 mm. Under the influence of repetitive loads, every implant will eventually bend or break. No implant, regardless of the manufacturer or technology, is immune to this. The risk increases with the patient’s body weight. This applies to all nails used for limb lengthening, regardless of the material from which they are made and the promises made by the manufacturer or physician.
At our center, we allow full weight-bearing on the limb only when an X-ray shows complete filling of the gap with bone tissue. At that point, the bone takes over the load and relieves the implant. During the lengthening process, we allow weight-bearing on the limb with the support of crutches or a walker, which allow the body’s weight to be transferred to the arms. The permitted weight-bearing level depends on several factors: the patient’s body weight, the diameter of the nail, and the bone being lengthened. For the Precice2 nail with the largest diameter (12.5 mm), we allow a load of up to 34 kg on each leg. This means that if the patient stands on both feet while supported by two crutches, they can bear a load of up to 68 kg. However, when walking or shifting body weight from one leg to the other, the patient MUST USE TWO CRUTCHES and limit the load to 34 kg with each step. During the distraction phase, the patient is NEVER allowed to walk with a single crutch, regardless of body weight. The same rule applies during the consolidation period, until the doctor allows the weight-bearing limit to be increased. The patient can check the weight-bearing level of the limb by standing on a home scale, leaning on the crutches, and trying to reach the required weight, e.g., 34 kg. For smaller-diameter nails, 10.7 mm and 8.5 mm, no more than 23 kg per leg is permitted.
Rehabilitation takes place at the Paley European Institute five times a week throughout the lengthening process under the supervision of a dedicated physical therapist. In addition, the patient performs rehabilitation exercises at home daily, at least three times a day, following the protocol provided by us.
During the consolidation phase, rehabilitation must continue, though with reduced frequency (2–3 times a week). We also adjust the scope and nature of the exercises during this time. In this phase, we place particular emphasis on motor training to accelerate the return to full activity.
The lengthening process is performed by the patient or a family member at home. The nail is lengthened by ¼ mm at a time, 4 times a day for the femur and 3 times a day for the tibia. In cases where both the femur and tibia are being lengthened simultaneously, the procedure is performed only 3 times a day. The entire process is facilitated by a special transmitter or “remote control,” the ERC (External Remote Control). Each patient is trained in the use of the ERC by our orthopedic technician until they become proficient. Each patient receives an ERC for their personal use. The device must be returned upon completion of the lengthening phase.
A follow-up visit with a doctor takes place every two weeks at the Paley European Institute. In addition, if a patient experiences any concerning symptoms, they can contact their Patient Coordinator by phone. Throughout the rehabilitation process, our physical therapists also continuously monitor the lengthening process in consultation with the medical team.
X-rays of each bone undergoing lengthening are taken every two weeks prior to a follow-up medical visit.
After reviewing the patient’s X-rays, Dr. Deszczyński or Dr. Albrewczyński will respond via
email with their interpretation of the findings and their opinion regarding the possibility of full weight-bearing on the limbs.
Full weight-bearing is usually possible 1–2 months after the completion of the distraction phase. Most patients can walk with full weight-bearing one month after the completion of a 5 cm femur lengthening and two months after the completion of a 5 cm tibia lengthening. In the case of an 8 cm femur lengthening, this is usually possible after
2 months.
Before resuming sports activities, the patient must first regain muscle function and strength. With intensive rehabilitation, it is possible to return to sports as early as six months after surgery. However, this is an individual matter and depends on the doctor’s assessment. Most patients can resume running approximately one month after receiving approval to stop using crutches. Other sports can be resumed approximately one month after starting to run. To accelerate our patients’ full return to sports, we have introduced a special functional training protocol at the Paley European Institute following limb lengthening.
Yes—all pins must be removed. The timing is not critical, but the pins are typically removed one or two years after the initial surgery. This is necessary because the pins are made of titanium or steel and release metal ions over the years, and also because they have moving parts. The Precice device is equipped with a rare-earth magnet. It is isolated from the body inside a waterproof chamber. There is a risk that, over the years, the chamber’s seal may fail, allowing the rare-earth magnet to come into contact with bodily fluids. Before this happens, it is advisable to have the device removed.
It is recommended to wait between six months and one year between procedures. Femur and tibia lengthening procedures can be performed at the same time; this option can be discussed with Dr. Deszczyński or
Dr. Albrewczyński.
There are many potential complications associated with limb-lengthening procedures. These are discussed in detail with the patient during the initial consultation and again during the preoperative visit. These include, among others: failure of bone union, limb length discrepancy, nerve damage due to stretching, muscle/tendon contractures leading to joint stiffness, and joint inflammation. Other possible complications include deep vein thrombosis and fat embolism. Incomplete union is rare. Excessive nerve tension may occur, which sometimes requires surgical nerve decompression. Tight muscles and tendons may require surgical lengthening. Such problems are unlikely, but if they do occur, the Paley European Institute is experienced in their diagnosis and prompt, appropriate treatment. Extension that is too slow or placement of the ERC controller in the wrong location (not directly over the magnet inside the nail) may contribute to premature union. If this occurs, another surgery is necessary to re-cut the bone to allow for further lengthening.
Most of our patients achieve excellent results without major complications. If complications do arise, treatment outcomes are usually good as well, provided they are diagnosed and treated promptly. The procedure requires long-term rehabilitation, and a return to full fitness—including sports activities—can take more than six months.
Limb-lengthening procedures should only be performed by experienced specialists. The Paley European Institute is one of the world’s most experienced centers in the field of limb lengthening. Our patients have come to us from many countries to take advantage of the comprehensive orthopedic therapies offered by our highly reputable team. At our Institute, the attending physician explains all available treatment options in detail and then tailors the treatment plan to the individual’s specific needs. Our patients receive comprehensive care from our entire team, which includes experienced orthopedic surgeons as well as specialized assistants, nurses, and physical therapists. Thanks to us, patients achieve the best possible results in limb lengthening for aesthetic purposes.
The PRECICE method is considered the safest primarily because of the minimized risk of infection, which is less than 1%, since the entire device is located inside the bone. Unlike traditional methods, the patient does not have to deal with frequent infections around wires that pass through the skin. A key safety feature is the unique design of the magnetically driven telescopic nail, which gives the doctor full control over the process. This means that in the event of complications, such as excessive soft tissue tension or pain, the process can be stopped at any time and even reversed by retracting the nail and shortening the limb to a safe length. Such precision drastically reduces the risk of permanent contractures and nerve damage, which can occur with conventional distraction.
Yes, our clinic offers a limb-shortening procedure using advanced PRECICE technology. Although these nails are commonly associated with limb lengthening, their bidirectional magnetic mechanism allows for equally precise and controlled bone shortening. This solution is particularly appreciated by patients with leg length discrepancies, as it allows them to achieve full body symmetry without the need for cumbersome and uncomfortable external braces.
Photo gallery